
Column Can Spinal Canal Stenosis Recur? A Thorough Explanation of Postoperative Life and Risk Management
December 26, 2025
Spinal canal stenosis, along with herniated discs, is one of the most common spinal disorders.
Spinal canal stenosis causes not only low back pain, but also pain and numbness in the lower extremities, as well as intermittent claudication — a condition in which pain develops in the buttocks or legs while walking, improves with rest, and then recurs when walking is resumed. These symptoms can significantly interfere with daily life.
In this article, we explain surgical treatment for lumbar spinal stenosis and postoperative rehabilitation, with a focus on recurrence risk and long-term management.
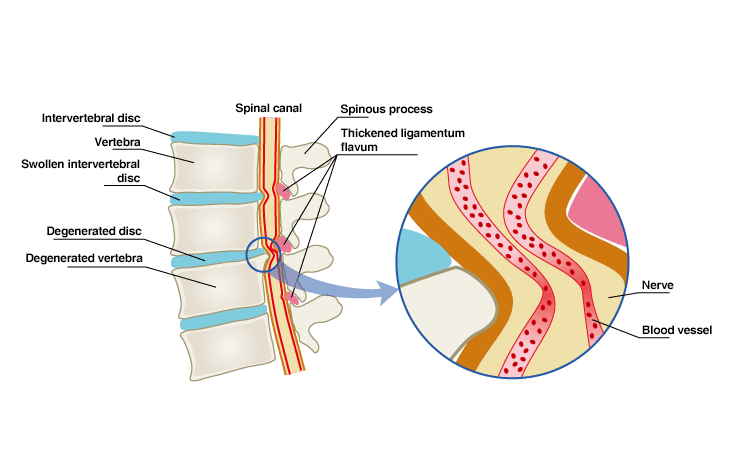
What is Spinal Canal Stenosis?
Spinal canal stenosis is a condition in which the pathway for nerves inside the spine (the spinal canal) becomes narrow.
Spinal canal narrowing can occur at any level of the spine, but it most commonly affects the lumbar region (lumbar spinal canal stenosis). It typically affects individuals over the age of 50 and tends to be more prevalent in men.
Symptoms of Lumbar Spinal Stenosis
When the spinal canal narrows and compresses the nerves, symptoms such as low back pain, leg pain, numbness, and muscle weakness may occur.
- Symptoms on the right side indicate compression of the right nerve root.
- Symptoms on the left side indicate compression of the left nerve root.
- Symptoms on both sides indicate compression of the cauda equina.
A typical symptom of spinal canal stenosis is intermittent claudication. This is a condition in which the lower limbs become numb or lose strength while walking, eventually making it impossible to continue. After sitting or squatting for a short period, symptoms improve and walking becomes possible again.
As stenosis progresses, the distance a patient can walk gradually decreases.
Treatment for Spinal Canal Stenosis: Surgical Procedures
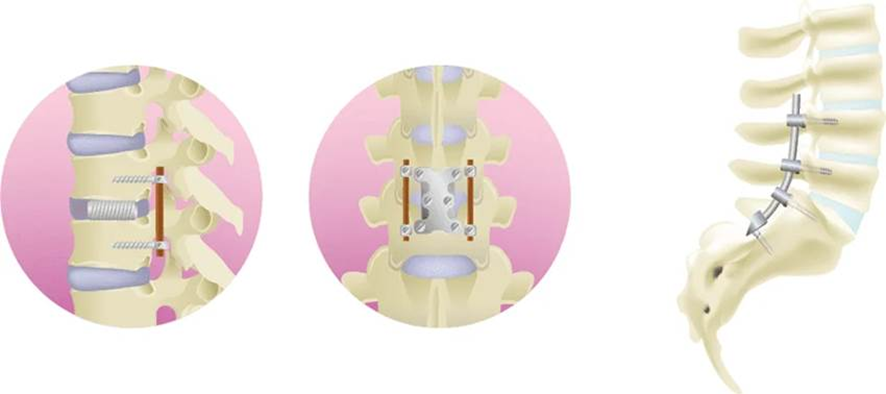
The most common surgeries for spinal canal stenosis are lumbar laminectomy and spinal fusion.
- Lumbar Laminectomy: Performed under general anesthesia, often using endoscopic techniques. A posterior incision is made, and part of the lamina and hypertrophied ligamentum flavum are removed to relieve nerve compression and widen the spinal canal.
- Spinal Fusion: Also performed under general anesthesia. An incision is made in the back, the degenerated intervertebral disc is removed, and a cage filled with bone (often harvested from the hip bone) is inserted. The vertebrae are then fixed in place using screws and rods. This is sometimes performed following a lumbar laminectomy.
Recurrence Rate After Surgery
It is not uncommon for the spinal canal to narrow again and symptoms to recur after a surgical procedure (decompression or fusion) has been performed for spinal canal stenosis. In such cases, reoperation is required at a relatively high rate, reported to be approximately between 10 to 23%. (*1)
Engaging in excessive movement immediately after the initial surgery increases the risk of needing reoperation in the future. Postoperative instability may occur, leading to facet joint degeneration or the development of spondylolisthesis. In these cases, the reoperation usually involves a fusion procedure.
(*1) : Atlas SJ, et al. Long-term outcomes of surgical and nonsurgical management of lumbar spine stenosis: 8 to 10 year results from the maine lumbar spine study. Spine, 2005, 30(8). Kim CH, et al. Reoperation rate after surgery for lumbar spinal stenosis without spondylolisthesis: a nationwide cohort study. Spine Journal, 2013, vol.13-10.
Life After Spinal Surgery
Surgical spine procedures require a period of hospitalization. At the earliest, one week is required, but in some cases, two weeks of hospitalization are necessary. The more surgical sites there are, the longer the hospitalization period will be.
Day after surgery: Starts with confirming movements such as getting out of bed and sitting. If postoperative progress is good, walking practice and daily activities will follow.
For the first two weeks, patients usually wear a lumbar brace (a corset) while performing light movements.
After 2 weeks: Desk work and driving a car become possible.
After 2 months: Heavy labor becomes feasible (abstain before this point).
After 3 months: Cycling and running may begin. Most sports may be resumed after 3 months, except for high-impact or contact sports that involve falling or collisions.
Minimally Invasive Procedures: The Florence Method & The Q-Florence Method
For lumbar spinal stenosis, Florence Method and Q-Florence Method are also available as treatment options.
These are low-risk, minimally invasive procedures performed under local anesthesia and sedation.
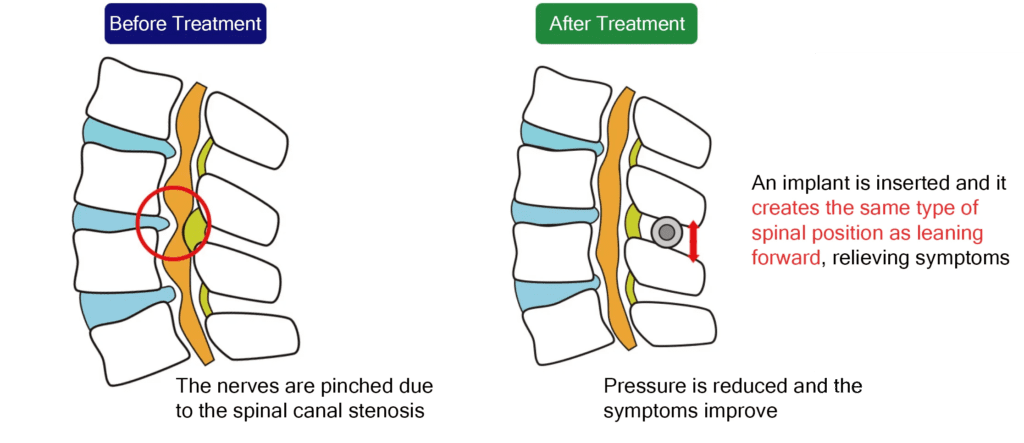
A percutaneous device is inserted to expand the narrowed spinal canal.
The device stabilizes the spine while preserving spinal rotation and flexion, expands the spinal canal, suppresses disc protrusion, and reduces hypertrophy of the ligamentum flavum. By enlarging the spinal canal, nerve compression is relieved and pain is reduced.
Recurrence Rate of Minimally Invasive Procedures
Because the Florence Method and Q-Florence Method are minimally invasive and low-risk, no reports of postoperative complications or symptom recurrence have been reported to date.
Life After Minimally Invasive Procedures
Patients can return home on the day of treatment
From the following day, light daily activities are permitted while avoiding excessive lumbar strain
After 7 days: light exercise may begin
After 14 days: yoga is permitted
Golf, sports, and heavy labor should be avoided for at least 1 month
Prevention of Spinal Canal Stenosis
Physical therapy is effective to prevent spinal canal stenosis or to prevent further progression if you have already been diagnosed.
◎ Exercise to Improve Spinal Mobility (Rotation)
The purpose of this exercise is to move the body flexibly and improve the movement from the pelvis to the spine.
1. Lie on your back with both knees bent
2. Focus on moving in this order: knees → pelvis → lower back
Consciously make the pelvis move first, followed by the lower back.
3. Perform this continuously and slowly for about 2 to 3 minutes without stopping the movement.

◎ Exercise to Improve Spinal Mobility (Core Control)
The purpose of this exercise is to enable spinal movement using abdominal strength.
Improving spinal mobility by using core abdominal strength can reduce lumbar load during actions such as standing up or walking.
1. Place your hands just below your navel.
2. Exhale through the nose while drawing the abdomen inward
3. While keeping that area hollowed inward, lift your buttocks only, while keeping your back on the floor.
4. Once the buttocks are raised, lower them slowly.
5. When lifting the buttocks, focus your awareness on the movement from the pelvis to the lumbar vertebrae (the spine in the lower back).

Our clinic also provides rehabilitation programs optimized for low back pain.
If you are suffering from spinal canal stenosis, please consider visiting our clinic for an examination.
Related Articles
Lumbar Spinal Canal Stenosis: What is Actually Happening to my Body?
Diagnosis and Treatment of Spinal Stenosis: Why Early Detection is Critical
The Different Symptoms of Spinal Canal Stenosis: If You Have Any of These, it’s a Red Flag!
Why Do the Symptoms of Spinal Stenosis Differ From Person to Person?
Self-Check for Lumbar Spinal Stenosis Severity
The Relationship Between Spinal Canal Stenosis and Leg Numbness
What are the Various Complications Possible With Spinal Stenosis?
